
Understanding Ultrasound Imaging
Ultrasound imaging, also known as sonography, is a non-invasive imaging technique that uses high-frequency sound waves to create real-time images of the body’s internal structures.
It is a safe and widely used diagnostic tool for assessing various medical conditions, including cervical cancer.
Ultrasound and Cervical Cancer
When it comes to cervical cancer, ultrasound can provide valuable information about the size, shape, and characteristics of the tumor. Although ultrasound is not typically the primary screening tool for cervical cancer, it is often used in conjunction with other diagnostic tests like Pap smears and colposcopy.
Transvaginal Ultrasound

For evaluating cervical cancer, transvaginal ultrasound is the preferred approach.
In this procedure, a small probe called a transducer is inserted into the vagina, allowing for a closer examination of the cervix and surrounding structures.
The transducer emits sound waves that bounce back from the tissues, creating a detailed image on the ultrasound monitor.
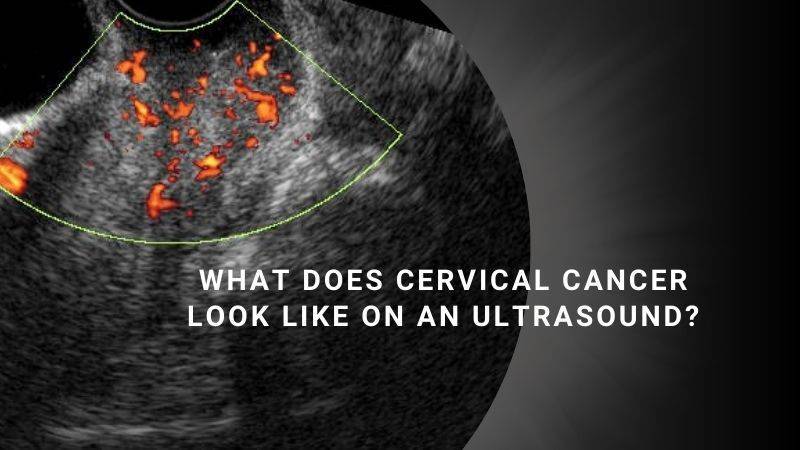
What Does Cervical Cancer Look Like on an Ultrasound?

On an ultrasound image, cervical cancer may appear as a mass or a growth in or around the cervix. The tumor can vary in size, shape, and texture.
The ultrasound can help determine if the mass is localized or has spread to nearby structures, such as the uterus or lymph nodes.
More Reliable Methods for Screening and Diagnosing Cervical Cancer

Pap Smear Test: A Pap smear, also known as a Pap test, is a routine screening procedure used to detect abnormal cervical cells that may indicate the presence of cervical cancer or precancerous changes.
HPV Test: The human papillomavirus (HPV) test detects the presence of high-risk strains of HPV, which can lead to cervical cancer. This test is often performed in conjunction with a Pap smear.
Colposcopy: If abnormalities are found during a Pap smear or HPV test, a colposcopy may be performed. This procedure involves examining the cervix and the surrounding tissues using a special magnifying instrument called a colposcope.
Biopsy: If suspicious areas are identified during a colposcopy, a biopsy may be recommended. This involves taking a small tissue sample from the cervix for further examination under a microscope to confirm the presence of cervical cancer.
How Often Should You Get Screened for Cervical Cancer?

The recommended screening guidelines may vary depending on your age and previous screening results.
Here are the general guidelines provided by reputable sources like the American Cancer Society and the Centers for Disease Control and Prevention (CDC):
Age 21: It is recommended to start cervical cancer screening with Pap tests from the age of 21, regardless of sexual activity or HPV vaccination history.
Ages 21 to 29: If Pap test results are normal, it is generally recommended to have a Pap test every three years during this age range.
Ages 30 to 65: There are a few options available for screening during this period:
a. Pap test only: If results are normal, it is typically advised to have a Pap test every three years.
b. HPV test only: Alternatively, an HPV test can be done alone, without a Pap test. If the HPV test results are negative, it is generally recommended to have an HPV test every five years.
c. Pap and HPV co-test: Another option is to have both a Pap test and an HPV test together. If both results are normal, it is typically advised to undergo testing every five years.
Age 65 and above: If you have had consistently normal screening results in recent years and are not at high risk, further testing may not be necessary. However, it is important to consult with your healthcare provider to determine the most appropriate course of action based on your individual circumstances.
Additionally, it is essential to be aware of any unusual changes or symptoms between screenings.
If you experience
- abnormal spotting or bleeding
- heavy menstrual periods
- unusual vaginal discharge
- pelvic pain, or bleeding or discomfort after sex
It is important to inform your doctor and seek medical attention promptly.
Remember, these are general guidelines, and individual situations may vary. It is crucial to have regular discussions with your healthcare provider to determine the most suitable screening schedule based on your age, medical history, and risk factors.